PROVIDENCE, R.I. [Brown University] — Say your aunt Betty is ready to be discharged from the hospital after a close call with congestive heart failure. Before she can go, she needs a care plan, and she’s relieved that she can return home with care from a home health agency. To choose an at-home provider, Betty and cousin Bob meet with a hospital case manager, but she only offers them a bare bones list of agency names, contact information, and the health insurance they accept.
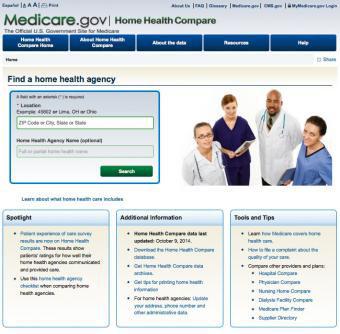
Which one offers the best care? A new study in the Journal of General Internal Medicine reports that the typical hospital case manager has little information to provide, even though state and federal quality reports are available on the Web. Through focus group interviews with 13 home health care consumers and 28 case managers at five Rhode Island hospitals, the researchers learned that no one was aware of state or federal home health care quality reports. Such reports include patient satisfaction ratings and data on outcomes such as hospital readmissions.
“It was a surprise to us,” said lead author Rosa Baier, newly appointed associate director of Brown University’s Center for Long Term Care Quality and Innovation and senior scientist at Healthcentric Advisors, which administers the study. Healthcentric Advisors is contracted by the Rhode Island Department of Health to run the state’s public reporting program. “Consumers expressed a desire to have access to more information that could inform their decision.”
Rhode Island may not be the only state where consumers aren’t seeing quality reports. The researchers informally surveyed another 40 case managers in five other states, finding that in seven out of every eight cases, those managers also shared only bare bones lists that provided no quality information from, or references to, online reports.
“Their process seems very similar to what is happening in Rhode Island,” Baier said.
Senior author Melissa Clark, professor of epidemiology in the Brown University School of Public Health, said the findings are notable in light of recent changes in health care policy and payments designed to reward quality in outcomes.
Clark, Baier, and their colleagues at Brown and Healthcentric Advisors conducted the study with a grant from the federal Agency for Healthcare Research and Quality.
Limited help
In addition to revealing that the reports were unknown, the focus group participants also yielded other insights about potential barriers to informing patients’ decision making about home health care. Most importantly, case managers reported feeling that federal laws or hospital policy prohibited them from answering patients’ questions about which agency they recommended or patients should choose.
“That’s all part of the Stark Laws,” said one case manager quoted in the study, referring (somewhat in error) to federal statutes designed to enforce ethics in health care provider referrals. “You can’t be perceived that we are giving business to a particular home health agency for a kick-back or anything like that.”
In fact, although case managers could share information if they had it, they felt constrained by the laws. Another case manager said, “I can’t tell you what everybody does and I can’t make decisions for you. ... I can’t help you choose.”
Several case managers also said they didn’t think there was much of a quality difference among providers or that quality wasn’t as important for at-home health as it is for residential nursing home care. Many case managers and some patients said they were, in fact, aware of state quality reports for nursing homes, but didn’t know about the reports on home care providers, Baier said.
Improving information
The authors’ research includes two more phases. The first focused on creating a Web-based quality report tailored to include what patients and family members said they would like to know.
The final phase, currently underway, involves conducting a randomized, controlled trial in which the investigators are testing whether offering the new quality report to consumers has an effect on their experience choosing home care and on the choices they make.
After conducting the focus groups, Baier and the Rhode Island Department of Health also began pushing updates about the existing quality reports to local hospitals instead of posting updates online for hospital staff to seek independently. Medicare and state public reporting programs should consider other ways of making hospital case managers more aware of the quality reports, Baier said, since case managers routinely help patients make decisions during hospital discharge and can make patients aware of existing quality reports if they themselves are aware of these resources.
“There’s a great opportunity if the right people are aware of the information,” Baier said. “Case managers don’t want to break the law and they do want to help patients make informed decisions. Having access to an unbiased source of information can take away that risk they feel when patients ask for their personal opinion.”
Clark said arming case managers with knowledge of the report could also improve care quality.
“Everyone involved in the care of a hospitalized patient, including the patient, family, healthcare providers, and hospital, wants the best possible outcomes for the patient.” Clark said. “Having information that hospital case managers can distribute about home health agencies beyond a name and telephone number may be a way to help patients and their families choose an agency that provides the highest quality of care for their particular health condition.”
In addition to Baier and Clark, the paper’s authors are Andrea Wysocki, Dr. Stefan Gravenstein, Emily Cooper and Vincent Mor.