PROVIDENCE, R.I. [Brown University] — Brown University sociologists have developed a device to gather more reliable data about risky sexual behavior among Ethiopian teenagers and young adults than conventional face-to-face interviews can produce. Simple, portable, low-cost, and low-tech, the group’s new nonverbal response card allows respondents to communicate nonverbally and confidentially during face-to-face interviews. Professors of sociology David Lindstrom and Dennis Hogan, and postdoctoral research associate Megan Klein Hattori published their findings in the December issue of Studies in Family Planning.
Successful programs to combat the spread of HIV/AIDS require accurate information about the prevalence of risky sexual behavior among populations. Obtaining that information can often be tricky due to intentional misreporting on sensitive topics. A number of innovations in questionnaire methodology have been developed to address reporting bias, but those techniques can be expensive, technically unreliable, and dependant on basic literacy.
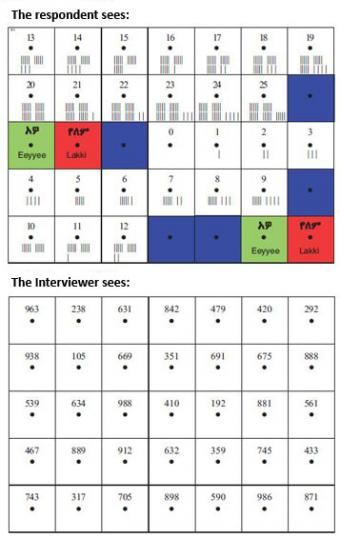
The group’s new nonverbal response card is an 8.5-by-11 inch laminated sheet of paper with a respondent side and an interviewer side. Each side is divided into 35 cells with a small hole punched through the center of each cell. On the respondent side of the card, the cells contain written and color-coded responses. The numeric responses, for questions such as the number of sexual partners or age at first sex, range from 0-25, marked with both a written number and vertical bars for tallying (for example, II for 2 and IIIII IIIII for 10). The non-numeric responses (yes, no, and does not apply) are written in local languages and also color-coded with green, red, and blue. On the interviewer side of the card, each cell contains a unique survey-specific three-digit number.

For sensitive portions of interviews, the respondent selects a card and holds it up. The interviewer asks the question and the respondent indicates the answer by inserting a stick through the hole of the appropriate cell. For example, the interviewer asks, “Have you ever had sexual intercourse? Point to green for yes, red for no.” The respondent pokes the stick through any of the green or red cells and the the interviewer records the three digit number of the cell through which the stick is protruding. The numbers are later entered into data files and decoded, which allows for full confidentiality.
The research team tested the card in a survey of 1,269 Ethiopian men and women aged 13 to 24. The adolescent and young adult respondents were from rural communities and small urban centers in southwestern Ethiopia, which is a predominantly Muslim population. The respondents were interviewed at home (often with parents or other family members nearby) on topics including aspirations, food insecurity, and HIV knowledge, as well as romantic relationships, sexual intercourse, and condom knowledge and use. One half of the study sample used the cards, while the other half gave traditional verbal responses to interviewers.
The researchers found that respondents were twice as likely to report having premarital sex when using a nonverbal response card. The effect of the response method on the willingness to report risk of acquiring HIV in the 12 months prior to the survey were “especially striking.” Virtually no respondents answering the questions verbally admitted to being at risk of acquiring HIV, compared to 3.8 percent of the respondents who used the card method.
The researchers found that young people over-report knowledge of condoms when they give verbal responses: About half of the single respondents giving verbal responses reported knowing where to obtain a condom, compared to only 37 percent of the single respondents in the card group.
“The difference in reported knowledge to access to condoms presents additional challenges for public health programs by suggesting that conventional survey estimates may significantly overestimate this knowledge, and most likely condom use as well, among subgroups who are often the target of outreach programs,” the authors wrote.
The response cards cost about $2 to produce, are highly portable and reliable, and are particularly useful in low-income rural settings where illiteracy is common.
“It’s clear that more sophisticated and costly survey technologies are not always the best solution when it comes to these types of surveys and questions,” said Lindstrom. “I hope this method is picked up and tried in research settings where sensitive questions are being asked.”
Lindstrom, Hogan, and Hattori are all affiliated with the Population Studies and Training Center at Brown. Their research group also included Tefera Belachew and Fasil Tessema of Jimma University in Ethiopia, and Craig Hadley of Emory University. This work was supported by the David and Lucile Packard Foundation, the Mellon Foundation, the Compton Foundation, and the National Institutes of Health.